


1Department of Medical Sciences and Human Oncology, Section of Dermatology, 2Department of Neuroscience and Mental Health, Section of Neurology, 3Department of Oncology, Section of Radiotherapy and 4Department of Laboratory Medicine, Section of Anatomic Pathology, University of Turin, Via Cherasco 23, IT-12124 Torino, Italy. E-mail: andrea93.agostini@gmail.com
#Shared co-first authorship. *Shared co-first senior authorship.
Accepted Apr 1, 2021; Epub ahead of print Apr 13, 2021
Acta Derm Venereol 2021; 101: adv00452.
doi: 10.2340/00015555-3798
Merkel cell carcinoma (MCC) is a rare aggressive skin cancer, the incidence of which is increasing rapidly (1). Various paraneoplastic syndromes have been associated with MCC, due to its neuroendocrine nature, and these could be the first manifestations of cancer (2–7). We report here a case of a patient whose diagnosis of MCC with unknown primary was made following the identification of 2 uncommon neurological disorders. This case report highlights the complexity of paraneoplastic syndrome associated with MCC and the importance of a multidisciplinary approach.
An otherwise healthy 59-year-old man was admitted to the neurology clinic at the emergency department due to rapidly worsening difficulties in walking, and limb weakness associated with ataxia, diplopy and nystagmus in the previous 2 weeks.
Radiological imaging, including high-resolution computed tomography (CT) and magnetic resonance imaging (MRI), did not disclose any significant abnormalities. Viral and bacterial serological tests were negative. Motor-nerve conduction studies showed post-exercise facilitation, and a qualitative assay for the presence of P/Q-type voltage-gated calcium channel antibodies was positive. These results led to a diagnosis of Lambert-Eaton myasthenic syndrome (LEMS) associated with manifestations of cerebellar degeneration. Symptomatic treatment with fampridine, a potassium channel blocker, was tried with partial improvement.
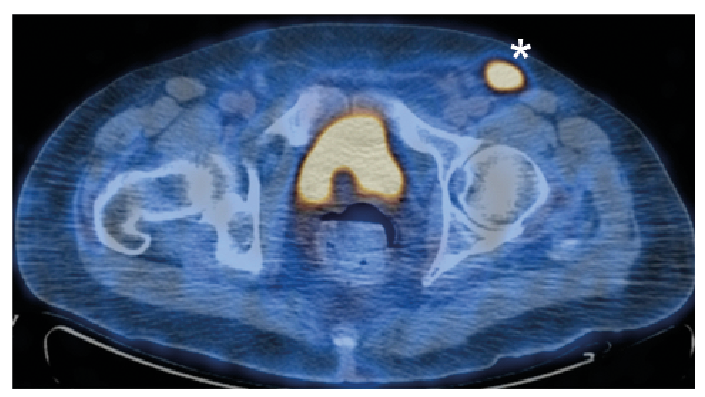
Positron emission tomography (PET; Fig. 1) revealed hyper-metabolic lesions in left inguinal lymph nodes. An excisional biopsy showed positive immunohistochemical reactions with anti-synaptophysin antibodies (Fig. 2A), cytokeratins AE1/AE3, cytokeratin 20 (Fig. 2B), and chromogranin A. MIB-1 proliferative activity was 70%; the presence of numerous mitoses (15/10 high-power field) and areas of necrosis was reported (Fig. 2C). These findings were consistent with a diagnosis of lymph node deposit of metastatic cells of Merkel cell carcinoma (MCC).
Fig. 1. Positron tomography scan showing enlarged left inguinal node (SUVmax 8.8, imaging acquired head-first).
Fig. 2. Histological appearance of the lymph node with positive immunohistochemical reactions with: (A) anti-synaptophysin antibodies (10x) and (B) cytokeratin 20 (20x). (C) Presence of numerous mitoses (15/10 high-power field) and areas of necrosis was reported (hematoxylin and eosin stain, 20x).
The clinical history was unremarkable regarding previous excisions or spontaneous regressions of skin lesions. A careful clinical and dermoscopic examination did not find any cutaneous lesions suggestive of MCC, and PET scan did not show any other hyper-metabolic lesions.
The multidisciplinary oncological committee opted for moderate hypofractionated radiotherapy with a total dose of 50 Gy, as the patient’s performance status did not allow a radical surgical treatment. A computed tomography (CT) scan performed 2 months later demonstrated remission of the disease.
After 6 months’ follow-up, the patient showed a partial improvement in walking, but persistence of ataxia, diplopy and nystagmus due to referable to a paraneoplastic cerebellar degeneration (PCD) in association with LEMS consequent to MCC with unknown primary.
MCC is a rare malignant neuroendocrine skin carcinoma associated with a high rate of local and distant metastases and poor prognosis. Typically, MCC is a primary carcinoma of the skin, but it can be detected in different sites without an apparent primary localization (1). Few cases of lymph node involvement by MCC with an unknown primary tumour have been reported in the medical literature. It remains unclear whether the nodal MCC is a primary tumour of the lymph node or a metastasis from an occult or regressed extranodal lesion (8).
The current case is of interest due to the association of 2 paraneoplastic disorders in a patient with unknown primary MCC. LEMS is an antibody-mediated disorder of the neuromuscular junction, while PCD is a consequence of autoimmune destruction of cerebellar Purkinje cells.
Paraneoplastic syndromes can be associated with MCC, although this is rarely reported (only 27 cases have been published to date in the English literature) (2–7). Of these, 8 patients presented with LEMS and 5 were affected by PCD associated with MCC. It should be noted that almost the half of the 27 cases described were secondary to MCC with unknown primitive. To our knowledge, the association of both LEMS and PCD with MCC has been described only in a patient with MCC metastasis in the axilla and unknown primary (7).
In the current, the first-line treatment considered would have been complete lymphadenectomy; however, after multidisciplinary discussion, this was not performed, due to patient’s general conditions (9). We therefore opted for radiotherapy, discarding the possibility of anti-PDL1 therapy due to the immune manifestations already present in the patient. Regarding the only slight improvement in the neurological symptoms, a possible explanation could be the current persistence of occult MCC neoplastic cells, or non-resolution of the paraneoplastic picture, following treatment of the underlying oncological disease.
This case report highlights the importance of multidisciplinary management; dermatologists should be aware of the possible paraneoplastic syndromes associated with MCC.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize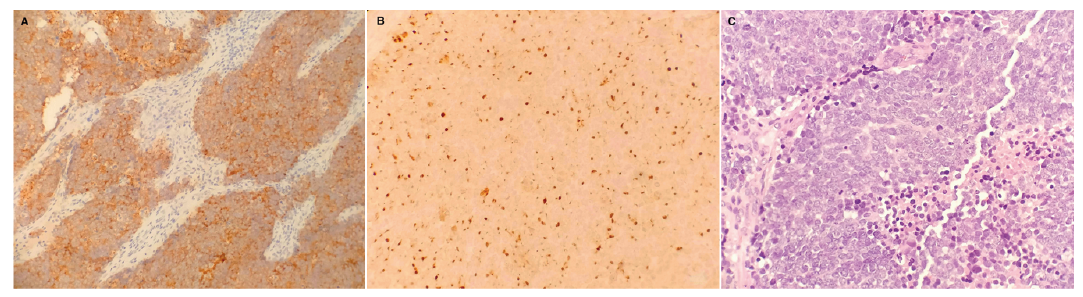 Click to show fullsize
Click to show fullsize